Dyspnea- This is a violation of breathing, which is accompanied by a change in its frequency and depth. As a rule, breathing with shortness of breath is rapid and shallow, which is a compensatory mechanism ( adjusting the body) in response to a lack of oxygen. Shortness of breath that occurs during inhalation is called inspiratory, shortness of breath during exhalation is called expiratory. It can also be mixed, that is, it can be found on both inhalation and exhalation. Subjectively, shortness of breath is felt as a lack of air, a feeling of squeezing the chest. Normally, shortness of breath can appear in a healthy person, in which case it is called physiological.
Physiological shortness of breath may appear in the following cases:
- as a reaction of the body to excessive physical exertion, especially if the body is not constantly subjected to physical exertion;
- at high altitudes, where conditions of hypoxia are created ( lack of oxygen);
- in confined spaces with an increased amount of carbon dioxide ( hypercapnia).
Depending on the etiology(causes of)shortness of breath can be of the following types:
- cardiac dyspnea;
- pulmonary dyspnea;
- shortness of breath as a result of anemia.
Doctors who can be consulted when shortness of breath occurs include:
- therapist;
- family doctor;
- cardiologist;
- pulmonologist.
How does a person breathe?
 Breathing is a physiological process during which gas exchange occurs, that is, the body receives oxygen from the external environment and releases carbon dioxide and other metabolic products. This is one of the most important functions of the body, since the vital activity of the body is maintained thanks to breathing. Breathing is a complex process that is carried out mainly with the help of the respiratory system.
Breathing is a physiological process during which gas exchange occurs, that is, the body receives oxygen from the external environment and releases carbon dioxide and other metabolic products. This is one of the most important functions of the body, since the vital activity of the body is maintained thanks to breathing. Breathing is a complex process that is carried out mainly with the help of the respiratory system. The respiratory system consists of the following organs:
- the cavity of the nose and mouth;
- larynx;
- trachea;
- bronchi;
- lungs.
Atmospheric air through the airways enters the lungs and further into the pulmonary alveoli. Gas exchange occurs in the alveoli, that is, carbon dioxide is released, and the blood is saturated with oxygen. Next, oxygenated blood is sent to the heart through the pulmonary veins, which flow into the left atrium. From the left atrium, blood goes to the left ventricle, from where it goes through the aorta to organs and tissues. Caliber ( the size) arteries, through which blood is carried throughout the body, moving away from the heart, gradually decreases to capillaries, through the membrane of which gases are exchanged with tissues.
The act of breathing consists of two stages:
- Inhale, in which atmospheric air enriched with oxygen enters the body. Inhalation is an active process involving the respiratory muscles.
- Exhalation, at which the release of air saturated with carbon dioxide occurs. When you exhale, the respiratory muscles relax.
Cardiac dyspnea
 Heart dyspnea is shortness of breath that develops as a result of heart pathologies. As a rule, cardiac dyspnea is chronic. Shortness of breath with heart disease is one of the most important symptoms. In some cases, depending on the type of shortness of breath, duration, physical activity, after which it appears, one can judge the stage of heart failure. Cardiac dyspnea is usually characterized by inspiratory dyspnea and frequent attacks of paroxysmal ( recurring) nocturnal shortness of breath.
Heart dyspnea is shortness of breath that develops as a result of heart pathologies. As a rule, cardiac dyspnea is chronic. Shortness of breath with heart disease is one of the most important symptoms. In some cases, depending on the type of shortness of breath, duration, physical activity, after which it appears, one can judge the stage of heart failure. Cardiac dyspnea is usually characterized by inspiratory dyspnea and frequent attacks of paroxysmal ( recurring) nocturnal shortness of breath. Causes of cardiac dyspnea
There are many reasons that can cause shortness of breath. These can be congenital diseases associated with genetic abnormalities, as well as acquired ones, the risk of which increases with age and depends on the presence of risk factors.The most common causes of cardiac dyspnea include:
- heart failure;
- acute coronary syndrome;
- hemopericardium, cardiac tamponade.
Heart failure is a pathology in which the heart, for certain reasons, is unable to pump the volume of blood that is necessary for the normal metabolism and functioning of organs and body systems.
In most cases, heart failure develops with such pathological conditions as:
- arterial hypertension;
- Ischemic heart disease ( cardiac ischemia);
- constrictive pericarditis ( inflammation of the pericardium, accompanied by its hardening and violation of the contraction of the heart);
- restrictive cardiomyopathy ( inflammation of the heart muscle with a decrease in its extensibility);
- pulmonary hypertension ( increased blood pressure in the pulmonary artery);
- bradycardia ( decrease in heart rate) or tachycardia ( increased heart rate) of various etiology;
- heart defects.
In the early stages of heart failure, shortness of breath may be absent. Further, with the progression of the pathology, shortness of breath appears with heavy exertion, with light loads, and even at rest.
Symptoms of heart failure associated with shortness of breath are:
- cyanosis ( bluish tint of the skin);
- cough, especially at night;
- hemoptysis ( hemoptysis) - coughing up sputum mixed with blood;
- orthopnea - rapid breathing in a horizontal position;
- nocturia - an increase in the formation of urine at night;
Acute coronary syndrome is a group of symptoms and signs that suggest myocardial infarction or unstable angina pectoris. Myocardial infarction is a disease that occurs as a result of an imbalance between myocardial oxygen demand and oxygen delivery, which as a result leads to necrosis of a portion of the myocardium. Unstable angina is an exacerbation of coronary artery disease that can lead to myocardial infarction or sudden death. These two conditions are combined into one syndrome due to the general pathogenetic mechanism and the difficulty of differential diagnosis between them at first. Acute coronary syndrome occurs in atherosclerosis and thrombosis of the coronary arteries, which cannot provide the myocardium with the required amount of oxygen.
The symptoms of acute coronary syndrome are considered to be:
- chest pain, which can also radiate to the left shoulder, left arm, lower jaw; pain usually lasts more than 10 minutes;
- shortness of breath, feeling short of breath;
- a feeling of heaviness behind the breastbone;
- blanching of the skin;
First aid for symptoms of acute coronary syndrome - sublingual nitroglycerin ( under the tongue), unbuttoning tight, chest-tight clothing, supplying fresh air and calling an ambulance.
Heart defects
Heart disease is a pathological change in the structures of the heart that leads to impaired blood flow. The blood flow is disturbed both in the large and in the pulmonary circulation. Heart defects can be congenital or acquired. They can relate to the following structures - valves, septa, vessels, walls. Congenital heart defects appear as a result of various genetic abnormalities, intrauterine infections. Acquired heart defects can occur against the background of infective endocarditis ( inflammation of the inner lining of the heart), rheumatism, syphilis.
Heart defects include the following pathologies:
- ventricular septal defect- This is an acquired heart disease, which is characterized by the presence of a defect in certain parts of the interventricular septum, which is located between the right and left ventricles of the heart;
- open oval window- a defect in the interatrial septum, which occurs due to the fact that there is no closure of the oval window, which is involved in the blood circulation of the fetus;
- open arterial ( botalls) duct, which in the prenatal period connects the aorta with the pulmonary artery, and during the first days of life should close;
- coarctation of the aorta- heart disease, which is manifested by a narrowing of the lumen of the aorta and requires cardiac surgery;
- heart valve failure- this is a type of heart defect in which it is impossible to completely close the valves of the heart and reverse blood flow occurs;
- valvular stenosis characterized by narrowing or fusion of the valve leaflets and disruption of normal blood flow.
Symptoms that are most common with heart defects are:
- dyspnea;
- cyanosis of the skin;
- pallor of the skin;
- loss of consciousness;
- lag in physical development;
Heart defects are diseases in which the condition can be alleviated with the help of therapeutic methods, but it can only be completely cured with the help of surgery.
Cardiomyopathy
Cardiomyopathy is a disease characterized by heart damage and manifested by hypertrophy ( an increase in the volume of muscle cells in the heart) or dilatation ( an increase in the volume of the heart chambers).
There are two types of cardiomyopathies:
- primary (idiopathic), the cause of which is unknown, but it is assumed that these may be autoimmune disorders, infectious factors ( viruses), genetic and other factors;
- secondary, which appears against the background of various diseases ( hypertension, intoxication, coronary heart disease, amyloidosis and other diseases).
The most common manifestations of cardiomyopathy are considered to be:
- shortness of breath;
- cough;
- blanching of the skin;
- increased fatigue;
- increased heart rate;
- dizziness.
Myocarditis
Myocarditis is myocardial damage ( heart muscle) predominantly of an inflammatory nature. The symptoms of myocarditis are shortness of breath, chest pain, dizziness, weakness.
Among the causes of myocarditis are:
- Bacterial, viral infections more often than other causes cause infectious myocarditis. The most common causative agents of the disease are viruses, namely Coxsackie virus, measles virus, rubella virus.
- Rheumatism, in which myocarditis is one of the main manifestations.
- Systemic diseases such as systemic lupus erythematosus, vasculitis ( inflammation of the blood vessel walls) lead to myocardial damage.
- Taking some medications ( antibiotics), vaccines, sera can also lead to myocarditis.
In order to prevent the appearance of myocarditis, it is necessary to treat infectious diseases in a timely manner, to reorganize chronic foci of infections ( caries, tonsillitis), rationally prescribe medications, vaccines and serums.
Pericarditis
Pericarditis is an inflammatory lesion of the pericardium ( pericardium). The causes of pericarditis are similar to those of myocarditis. Pericarditis is manifested by prolonged chest pain ( which, unlike acute coronary syndrome, do not disappear when taking nitroglycerin), fever, severe shortness of breath. With pericarditis, due to inflammatory changes in the pericardial cavity, adhesions can form, which can then grow together, which significantly complicates the work of the heart.
With pericarditis, shortness of breath is often formed in a horizontal position. Shortness of breath with pericarditis is a constant symptom and it does not disappear until the cause of the occurrence is eliminated.
Heart tamponade
Cardiac tamponade is a pathological condition in which fluid accumulates in the pericardial cavity and hemodynamics is impaired ( movement of blood through the vessels). The fluid in the pericardial cavity compresses the heart and restricts heartbeat.
Cardiac tamponade can appear as acute ( with injuries), and in chronic diseases ( pericarditis). It manifests itself as excruciating shortness of breath, tachycardia, and a decrease in blood pressure. Cardiac tamponade can cause acute heart failure, shock. This pathology is very dangerous and can lead to a complete cessation of cardiac activity. Therefore, timely medical intervention is of utmost importance. On an emergency basis, pericardial puncture and removal of pathological fluid are performed.
Diagnosis of cardiac dyspnea
Shortness of breath, being a symptom that can occur in pathologies of various organs and systems, requires careful diagnosis. Research methods for the diagnosis of shortness of breath are very diverse and include examination of the patient, paraclinical ( laboratory) and instrumental studies.The following methods are used to diagnose shortness of breath:
- physical examination ( conversation with the patient, examination, palpation, percussion, auscultation);
- ultrasonography ( transesophageal, transthoracic);
- chest x-ray;
- CT ( CT scan);
- MRI ( );
- ECG ( electrocardiography), ECG monitoring;
- cardiac catheterization;
- veloergometry.
The very first step in making a diagnosis is taking an anamnesis ( that is, questioning the patient), and then examination of the patient.
When collecting an anamnesis, you should pay attention to the following information:
- A characteristic of shortness of breath, which may be inspiratory, expiratory, or mixed.
- The intensity of shortness of breath can also indicate a certain pathological condition.
- Hereditary factor. The likelihood of heart disease, if the parents had them, is several times higher.
- The presence of various chronic heart diseases.
- You should also pay attention to the time of the onset of shortness of breath, its dependence on body position, on physical activity. If shortness of breath occurs during exercise, the intensity of the exercise should be checked.
Percussion of the heart gives information about an increase in the boundaries of the heart, which occurs due to the phenomena of hypertrophy or dilatation. Normally, with percussion, the sound is dull. A change and displacement of the boundaries of cardiac dullness speaks of cardiac pathologies or pathologies of other organs of the mediastinum.
The next step in the examination of the patient is auscultation ( listening). Auscultation is performed using a phonendoscope.
With the help of auscultation of the heart, the following changes can be determined:
- weakening of the sonority of heart tones ( myocarditis, myocardial infarction, cardiosclerosis, valve insufficiency);
- strengthening the sonority of heart tones ( atrioventricular stenosis);
- split heart sounds ( mitral stenosis, non-simultaneous closure of the bicuspid and tricuspid valves);
- pericardial friction noise ( dry or effusive pericarditis, after myocardial infarction);
- other noises ( in case of insufficiency of valves, stenosis of holes, stenosis of the aortic opening).
A complete blood count is a laboratory test method that allows you to assess the cellular composition of the blood.
In the general analysis of blood for cardiac pathologies, changes in the following indicators are of interest:
- Hemoglobin- It is a component of red blood cells that is involved in the transfer of oxygen. If the level of hemoglobin is low, this indirectly indicates that there is a lack of oxygen in the tissues, including the myocardium.
- Leukocytes... Leukocytes can be increased in the event of an infectious process in the body. An example is infective endocarditis, myocarditis, pericarditis. Sometimes leukocytosis ( increased leukocyte count) is observed with myocardial infarction.
- Erythrocytes often lowered in patients with chronic heart disease.
- Platelets participate in blood clotting. An increased number of platelets can be with a blockage of blood vessels, with a decrease in the level of platelets, bleeding is observed.
- ESR () is a nonspecific factor in the inflammatory process in the body. An increase in ESR occurs with myocardial infarction, with infectious heart disease, rheumatism.
A biochemical blood test is also informative in the case of diagnosing the causes of shortness of breath. A change in some indicators of a biochemical blood test indicates the presence of heart disease.
To diagnose the causes of cardiac dyspnea, the following biochemical parameters are analyzed:
- Lipidogram, which includes such indicators as lipoproteins, cholesterol, triglycerides. This indicator indicates a disturbance in lipid metabolism, the formation of atherosclerotic plaques, which, in turn, are a factor leading to most heart diseases.
- AST (aspartate aminotransferase). This enzyme is found in large quantities in the heart. Its increase indicates the presence of damage to the muscle cells of the heart. As a rule, AST is increased during the first days after myocardial infarction, then its level may be normal. By how much the level of AST is increased, one can judge the size of the area of necrosis ( cell death).
- LDH (lactate dehydrogenase). For the analysis of cardiac activity, the general level of LDH is important, as well as the LDH-1 and LDH-2 fractions. An increased level of this indicator indicates necrosis in the muscle tissue of the heart during myocardial infarction.
- KFK (creatine phosphokinase) is a marker of acute myocardial infarction. Also, CPK can be increased with myocarditis.
- Troponin Is a protein that is an integral part of cardiomyocytes and is involved in heart contraction. An increase in troponin levels indicates damage to myocardial cells in acute myocardial infarction.
- Coagulogram (blood clotting) indicates the risk of blood clots and pulmonary embolism.
- Acid phosphatase increases in patients with myocardial infarction with severe course and the presence of complications.
- Electrolytes (K, Na, Cl, Ca) increase in violation of the rhythm of cardiac activity, cardiovascular failure.
The general analysis of urine does not give an accurate description and localization of heart diseases, that is, this research method does not indicate specific signs of heart disease, but it can indirectly indicate the presence of a pathological process in the body. A general urinalysis is prescribed as a routine research method.
If you suspect dyspnea of a cardiac nature, X-ray examination is one of the most important and informative.
X-ray signs that speak of cardiac pathology and pathology of the vessels of the heart are:
- The size of the heart. An increase in the size of the heart can be noted with myocardial hypertrophy or dilatation of the chambers. It can occur with heart failure, cardiomyopathy, hypertension, coronary heart disease.
- Shape, configuration of the heart. You may notice an increase in the chambers of the heart.
- Saccular protrusion of the aorta with aneurysm.
- Accumulation of fluid in the pericardial cavity during pericarditis.
- Atherosclerotic lesion of the thoracic aorta.
- Signs of heart disease.
- Congestion in the lungs, basal infiltration in the lungs with heart failure.
CT scan of the heart and blood vessels
Computed tomography is a method of layer-by-layer examination of internal organs using X-rays. CT is an informative method that allows you to detect various pathologies of the heart, and also allows you to determine the possible risk of coronary heart disease ( cardiac ischemia) according to the degree of calcification ( deposition of calcium salts) coronary arteries.
Computed tomography can detect changes in the following structures of the heart:
- the condition of the coronary arteries - the degree of calcification of the coronary arteries ( by volume and mass of calcifications), stenosis of the coronary arteries, coronary shunts, coronary artery anomalies;
- aortic diseases - aortic aneurysm, aortic dissection, measurements required for aortic prosthetics can be taken;
- the state of the heart chambers - fibrosis ( overgrowth of connective tissue), dilatation of the ventricle, aneurysm, thinning of the walls, the presence of masses;
- changes in the pulmonary veins - stenosis, abnormal changes;
- with the help of CT, almost all heart defects can be detected;
- pathology of the pericardium - constrictive pericarditis, thickening of the pericardium.
MRI ( Magnetic resonance imaging) Is a very valuable method for studying the structure and functions of the heart. MRI is a method for examining internal organs based on the phenomenon of magnetic nuclear resonance. MRI can be performed both with contrast ( the introduction of a contrast agent for better tissue visualization), and without it, depending on the objectives of the study.
An MRI scan provides the following information:
- assessment of the functions of the heart, valves;
- the degree of myocardial damage;
- thickening of the walls of the myocardium;
- heart defects;
- diseases of the pericardium.
MRI is contraindicated in the presence of a pacemaker and other implants ( prostheses) with metal parts. The main advantages of this method are high information content and the absence of patient exposure.
Ultrasonography
Ultrasound is a method of examining internal organs using ultrasonic waves. For the diagnosis of heart disease, ultrasound is also one of the leading methods.
Ultrasound has a number of significant advantages:
- non-invasiveness ( no tissue damage);
- harmlessness ( no irradiation);
- low cost;
- fast results;
- high information content.
The following types of ultrasound examination are used to diagnose cardiac pathologies:
- Transthoracic echocardiography... In transthoracic echocardiography, the ultrasound transducer is placed on the surface of the skin. Different images can be obtained by changing the position and angle of the sensor.
- Transesophageal ( transesophageal) echocardiography... This type of echocardiography allows you to see things that can be difficult to see with transthoracic echocardiography due to the presence of obstructions ( adipose tissue, ribs, muscles, lungs). In this examination, the probe passes through the esophagus, which is key, since the esophagus is in the immediate vicinity of the heart.
ECG
An electrocardiogram is a method for graphically recording the electrical activity of the heart. ECG is an extremely important research method. With its help, you can detect signs of cardiac pathology, signs of a previous myocardial infarction. ECG is performed using an electrocardiograph, the results are issued immediately on the spot. A qualified doctor then conducts a thorough analysis of the ECG results and draws conclusions about the presence or absence of characteristic signs of pathology.
An ECG is done both once, and the so-called daily ECG monitoring ( by Holter). This method is used to continuously record an ECG. At the same time, physical activity is recorded, if any, the appearance of pain. The procedure usually lasts 1 to 3 days. In some cases, the procedure takes much longer - months. In this case, the sensors are implanted under the skin.
Cardiac catheterization
The Seldinger method of cardiac catheterization is more commonly used. The course of the procedure is monitored by a special camera. Local anesthesia is preliminarily performed. If the patient is restless, a sedative may also be given. A special needle is used to puncture the femoral vein, then a guide is inserted through the needle, which reaches the inferior vena cava. Next, a catheter is put on the guide wire, which is inserted into the right atrium, from where it can be inserted into the right ventricle or pulmonary trunk, and the guide wire is removed.
Cardiac catheterization allows you to:
- accurate measurement of systolic and diastolic pressure;
- oximetric analysis of blood obtained through a catheter ( determination of blood oxygen saturation).
Coronary angiography
Coronary angiography is a method for examining coronary ( coronal) arteries of the heart using X-rays. Coronary angiography is performed using catheters through which a contrast agent is injected into the coronary arteries. After the injection, the contrast agent completely fills the lumen of the artery, and with the help of an X-ray machine, several images are taken in different projections, which allow you to assess the state of the vessels.
Bicycle ergometry ( Stress ECG)
Bicycle ergometry is a research method that is performed using a special installation - a bicycle ergometer. A bicycle ergometer is a special type of exercise machine that can accurately dose physical activity. The patient sits on the ergometer, on the arms and legs ( possibly on the back or shoulder blades) electrodes are fixed, with the help of which the ECG is recorded.
The method is quite informative and allows you to assess the body's tolerance to physical activity and establish the permissible level of physical activity, identify signs of myocardial ischemia, evaluate the effectiveness of treatment, and determine the functional class of exertional angina.
Contraindications to cycling ergometry are:
- acute myocardial infarction;
- pulmonary embolism;
- unstable angina;
- late pregnancy;
- atrioventricular block 2 degree ( violation of the conduction of an electrical impulse from the atria to the ventricles of the heart);
- other acute and serious illnesses.
Treating cardiac dyspnea
Treatment of shortness of breath, first of all, should be aimed at eliminating the causes of its occurrence. Without knowing the causes of shortness of breath, it is impossible to fight it. In this regard, correct diagnosis is very important.In treatment, both pharmaceuticals and surgical interventions and traditional medicine can be used. In addition to the basic course of treatment, adherence to the diet, daily regimen and lifestyle adjustments are very important. It is recommended to limit excessive exercise, stress, treatment of heart disease and the risk factors leading to them.
Treatment of cardiac dyspnea is etiopathogenetic, that is, it is aimed at the causes and mechanism of its occurrence. Thus, to eliminate cardiac dyspnea, it is necessary to fight heart disease.
Groups of drugs used to treat heart dyspnea
| Group of drugs | Group representatives | Mechanism of action |
| Diuretics
(diuretics) |
| Eliminate edema, reduce blood pressure and stress on the heart. |
| ACE inhibitors
(angiotensin converting enzyme) |
| Vasoconstrictor, hypotensive action. |
| Angiotensin receptor blockers |
| Antihypertensive effect. |
| Beta blockers |
| Antihypertensive effect, reduction of heart rate and strength. |
| Aldosterone antagonists |
| Diuretic, antihypertensive, potassium-sparing action. |
| Cardiac glycosides |
| Cardiotonic action, normalize metabolic processes in the heart muscle, eliminate congestion. |
| Antiarrhythmic drugs |
| Normalization of the heart rate. |
Oxygen therapy is also recommended. Oxygen therapy is usually carried out in a hospital setting. Oxygen is supplied through a mask or special tubes, and the duration of the procedure is determined individually in each case.
Alternative treatments for shortness of breath include the following:
- Hawthorn normalizes blood circulation, has a tonic effect, hypotonic effect, lowers cholesterol levels. You can make tea, juice, infusion, balm from hawthorn.
- Fish fat helps to reduce heart rate, helps in the prevention of heart attacks.
- Mint, lemon balm have a sedative, vasodilator, hypotensive, anti-inflammatory effect.
- Valerian it is used for strong palpitations, pain in the heart, has a calming effect.
- Calendula helps with tachycardia, arrhythmias, hypertension.
Surgical treatments for cardiac dyspnea include the following:
- Coronary artery bypass grafting Is an operation aimed at restoring normal blood flow in the coronary arteries. This is done with shunts, which allow you to bypass the affected or narrowed area of the coronary artery. For this, a section of a peripheral vein or artery is taken and sutured between the coronary artery and the aorta. Thus, blood flow is restored.
- Valve replacement, valve restoration- this is the only type of operations with which you can radically ( fully) eliminate heart defects. Valves can be natural ( biological material, human or animal) and artificial ( synthetic materials, metals).
- Pacemaker Is a special device that supports cardiac activity. The device consists of two main parts - a generator of electrical impulses and an electrode, which transmits these impulses to the heart. Cardiac pacing can be external ( however, this method is now used quite rarely.) or internal ( permanent pacemaker implantation).
- Heart transplant... This method is the most extreme and, at the same time, the most difficult. Heart transplantation is performed at a time when it is no longer possible to cure the disease and maintain the patient's condition by any other methods.
Pulmonary dyspnea
 Pulmonary dyspnea is a disorder of depth and frequency of breathing associated with diseases of the respiratory system. With pulmonary dyspnea, air is obstructed, which rushes into the alveoli ( the end part of the breathing apparatus, has the shape of a bubble), insufficient oxygenation occurs ( oxygen saturation) blood, and characteristic symptoms appear.
Pulmonary dyspnea is a disorder of depth and frequency of breathing associated with diseases of the respiratory system. With pulmonary dyspnea, air is obstructed, which rushes into the alveoli ( the end part of the breathing apparatus, has the shape of a bubble), insufficient oxygenation occurs ( oxygen saturation) blood, and characteristic symptoms appear. Causes of pulmonary dyspnea
Pulmonary dyspnea can appear as a result of inflammatory diseases of the lung parenchyma, the presence of foreign bodies in the airways and other pathologies of the respiratory system.The conditions that most commonly lead to pulmonary dyspnea are:
- pneumothorax;
- hemothorax;
- pulmonary embolism;
- aspiration.
Chronic obstructive pulmonary disease is a disease characterized by a partially reversible and progressive obstruction of airflow in the airways due to an inflammatory process.
The most common causes of COPD are:
- Smoking... 90% of COPD cases are caused by smoking ( this also includes secondhand smoke);
- Pollution of atmospheric air and indoor air with various harmful substances (dust, pollution by substances emitted by street transport and industrial enterprises);
- Recurrent ( frequently recurring) infections bronchi and lungs often lead to exacerbation and progression of COPD;
- Frequent infections respiratory tract in childhood.
The main symptoms of COPD are:
- Cough at an early stage it appears rarely, with the progression of the disease it becomes chronic.
- Sputum initially released in small amounts, then its amount increases, it becomes viscous, purulent.
- Dyspnea- this is the latest symptom of the disease, it can appear several years after the onset of the disease, at first it appears only with intense physical exertion, then it appears during normal exertion. Shortness of breath, usually of a mixed type, that is, both on inspiration and on expiration.
Bronchial asthma
Bronchial asthma is a chronic inflammatory disease of the airways that is characterized by recurrent attacks of suffocation. The number of patients with asthma is about 5-10% of the population.
The reasons for the appearance of bronchial asthma include:
- a hereditary factor that occurs in about 30% of cases;
- allergic substances in the environment ( pollen, insects, mushrooms, animal hair);
- occupational factors in the workplace ( dust, harmful gases and vapors).
The most typical manifestations of bronchial asthma are:
- periodic occurrence of episodes of shortness of breath;
- cough;
- a feeling of discomfort in the chest;
- the appearance of phlegm;
- panic.
Emphysema of the lungs
Emphysema of the lungs is an irreversible expansion of the air space of the distal bronchioles as a result of destructive changes in their alveolar walls.
Among the reasons for the appearance of pulmonary emphysema, there are 2 main factors:
- COPD;
- deficiency of alpha-1-antitrypsin.
The main symptoms of emphysema are:
- dyspnea;
- sputum;
- cough;
- cyanosis;
- "Barrel-shaped" chest;
- expansion of the intercostal spaces.
Pneumonia
Pneumonia is an acute or chronic inflammation of the lungs that affects the alveoli and / or interstitial tissue of the lungs. Every year, about 7 million cases of pneumonia are fatal worldwide.
Pneumonia is mainly caused by various microorganisms and is an infectious disease.
The most common pathogens of pneumonia are the following microorganisms:
- Pneumococcus;
- respiratory viruses ( adenovirus, influenza virus);
- legionella.
The most common symptoms of pneumonia are:
- acute onset with an increase in temperature;
- cough with profuse expectoration;
- dyspnea;
- headache, weakness, malaise;
- chest pain.
Pneumothorax
Pneumothorax is an accumulation of air in the pleural space. The pneumothorax can be open or closed, depending on the presence of communication with the environment.
Pneumothorax can occur in the following cases:
- Spontaneous pneumothorax which occurs most frequently. Typically, spontaneous pneumothorax is caused by rupture of blisters with emphysema of the lung.
- Injury- penetrating ( penetrating) chest wounds, rib fractures.
- Iatrogenic pneumothorax (medical-related) - after pleural puncture, operations on the chest, catheterization of the subclavian vein.
The clinical manifestations of pneumothorax are:
- stitching pain in the affected part of the chest;
- dyspnea;
- asymmetric chest movements;
- pale or bluish tinge of the skin;
- coughing fits.
Hemothorax is a collection of blood in the pleural space. The pleural cavity with an accumulation of blood compresses the lung, makes it difficult to breathe and contributes to the displacement of the mediastinal organs.
Hemothorax appears as a result of the following factors:
- trauma ( penetrating chest wounds, closed injuries);
- medical manipulations ( after surgery, puncture);
- pathology ( tuberculosis, cancer, abscess, aortic aneurysm).
Symptoms characteristic of hemothorax are:
- pain in the chest, aggravated by coughing or breathing;
- dyspnea;
- forced sitting or semi-sitting position ( to alleviate the condition);
- tachycardia;
- pallor of the skin;
- fainting.
Pulmonary embolism
Pulmonary embolism is a blockage of the lumen of the pulmonary artery by emboli. An embolus can be a thrombus ( the most common cause of embolism), fat, tumor tissue, air.
Clinically, pulmonary embolism is manifested by the following symptoms:
- shortness of breath ( the most common symptom);
- tachycardia;
- severe chest pain;
- cough, hemoptysis ( hemoptysis);
- fainting, shock.
Pulmonary embolism can lead to pulmonary infarction, acute respiratory failure, instant death. In the initial stages of the disease, with timely medical care, the prognosis is quite favorable.
Aspiration
Aspiration is a condition characterized by the penetration of foreign bodies or liquid into the airways.
Aspiration is manifested by the following symptoms:
- expiratory dyspnea;
- harsh cough;
- suffocation;
- loss of consciousness;
- noisy breathing heard from a distance.
Diagnosis of pulmonary dyspnea
Diagnosing pulmonary dyspnea may seem straightforward at first. However, the purpose of diagnosis in this case is not only to identify the presence of a disease of the respiratory system, but also the form, stage, course of the disease and prognosis. Only a correct diagnosis can become the basis for adequate therapy.Pulmonary dyspnea is diagnosed using the following methods:
- physical examination;
- general blood analysis;
- general urine analysis;
- blood chemistry;
- determination of the level of D-dimers in the blood;
- chest x-ray;
- CT, MRI;
- scintigraphy;
- pulse oximetry;
- bodyplethysmography;
- spirometry;
- sputum examination;
- bronchoscopy;
- laryngoscopy;
- thoracoscopy;
- Ultrasound of the lungs.
The first step in making a diagnosis of pulmonary dyspnea is taking a history and examining the patient.
When collecting anamnesis, the following factors are of great importance:
- age;
- the presence of chronic pulmonary diseases;
- conditions at the workplace, since a large number of lung diseases occur due to the inhalation of harmful substances and gases during work;
- smoking is an absolute risk factor for lung disease;
- decreased immunity ( the body's defenses) when the body is unable to fight pathogenic factors;
- heredity ( bronchial asthma, tuberculosis, cystic fibrosis).
When examining a patient, you should pay attention to the following details:
- Skin color... Skin color can be pale or bluish, reddish ( hyperemia).
- Compelled position... With pleural effusion, lung abscess ( unilateral lesions) the patient tries to lie on the affected side. With an attack of bronchial asthma, the patient sits or stands and leans on the edge of a bed, table, chair.
- Chest shape... "Barrel-shaped" chest can be with emphysema. An asymmetric chest is found in unilateral lesions.
- Drumstick fingers appear with prolonged respiratory failure.
- Respiration characteristic- an increase or decrease in the frequency of respiratory movements, shallow or deep, arrhythmic breathing.
After palpation, start percussion ( tapping). With percussion, the lower border of the lungs, the apex of the lung is determined, the percussion sound is compared to the right and left. Normally, the percussion sound in the area of the lungs is sonorous and clear. With pathological changes, a clear pulmonary sound is replaced by a tympanic, dull, boxed sound.
Auscultation of the lungs is performed while sitting or standing. At the same time, the main respiratory sounds are heard, additional ( pathological) breathing sounds ( wheezing, crepitus, pleural rub).
General blood analysis
In the general analysis of blood, there are a number of indicators that are characterized by changes in pulmonary diseases.
A complete blood count (CBC) provides the following information that is important in diagnosing shortness of breath:
- Anemia- in case of pulmonary diseases, it is established due to the phenomenon of hypoxia.
- Leukocytosis- purulent lung diseases, infectious diseases of the respiratory tract ( bronchitis, pneumonia).
- Increased ESR ( erythrocyte sedimentation rate) indicates the presence of inflammatory diseases.
A general urine test, as well as a general blood test, is prescribed as a routine research method. He does not directly inform about any pulmonary disease, however, the following indicators can be detected - albuminuria, erythrocyturia, cylindruria, azotemia, oliguria.
Blood chemistry
A biochemical blood test is a very important method of laboratory research, the results of which make it possible to judge the state of various organs. A biochemical blood test allows you to detect active and latent diseases, inflammatory processes
For pulmonary diseases, the following indicators of a biochemical blood test are important:
- Total protein... In diseases of the respiratory system, it often decreases.
- Albumin-globulin ratio, in which changes occur in inflammatory lung diseases, namely, the amount of albumin decreases and the amount of globulins increases.
- CRB ( C-reactive protein) increases with inflammatory and degenerative diseases of the lungs.
- Haptoglobin (a protein that is found in blood plasma and binds hemoglobin) increases with pneumonia and other inflammatory diseases.
D-dimer level
D-dimer is a component of fibrin protein that is involved in blood clots. An increase in D-dimers in the blood indicates the process of excessive thrombus formation, although it does not indicate the exact location of the thrombus. The most common causes of an increase in D-dimers are pulmonary embolism, malignant neoplasms. If this indicator is normal, pathology is not excluded, since there is a possibility of obtaining false negative results.
Chest x-ray
Chest X-ray is the most common X-ray examination.
The list of diseases detected by radiography is extensive and includes the following:
- pneumonia;
- tumors;
- bronchitis;
- pneumothorax;
- pulmonary edema;
- trauma;
- other.
Respiratory system diseases can be detected by the following signs:
- decreased transparency of lung tissue;
- darkening of the pulmonary fields is the main radiological sign of pneumonia ( associated with inflammatory changes in the lung tissue), atelectasis;
- increased pulmonary pattern - COPD, tuberculosis, pneumonia;
- expansion of the root of the lung - chronic bronchitis, tuberculosis, expansion of the pulmonary arteries;
- foci of pneumosclerosis in COPD, chronic bronchitis, atelectasis, pneumoconiosis;
- smoothness of the costophrenic angle - pleural effusion;
- a cavity with a horizontal fluid level is characteristic of a lung abscess.
CT and MRI of the lungs are among the most accurate and informative methods. With these methods, a wide variety of lung diseases can be detected.
Thus, the following diseases can be diagnosed using CT and MRI:
- tumors;
- tuberculosis;
- pneumonia;
- pleurisy;
- swollen lymph nodes.
Scintigraphy is a research method that consists in introducing radioactive isotopes into the body and analyzing their distribution in various organs. Scintigraphy mainly detects pulmonary embolism.
The procedure is carried out in two stages:
- Blood supply scintigraphy... The labeled radioactive substance is injected intravenously. When disintegrating, the substance emits radiation, which is recorded by a camera and visualized on a computer. The absence of radiation indicates the presence of an embolism or other pulmonary disease.
- Ventilation scintigraphy... The patient inhales a radioactive substance, which, along with the inhaled air, spreads through the lungs. If an area is found where the gas does not enter, this indicates that something is an obstacle to the entry of air ( swelling, fluid).
Pulse Oximetry
Pulse oximetry is a diagnostic method for determining blood oxygen saturation. Normally, oxygen saturation should be 95 - 98%. With a decrease in this indicator, they speak of respiratory failure. Manipulation is performed using a pulse oximeter. This device is fixed on a finger or toe and calculates the content of oxygenated ( oxygenated) hemoglobin and pulse rate. The device consists of a monitor and a sensor that detects pulsation and provides information to the monitor.
Bodyplethysmography
Bodyplethysmography is a more informative method compared to spirography. This method allows you to analyze in detail the functional capacity of the lungs, to determine the residual volume of the lungs, the total capacity of the lungs, the functional residual of the lungs, which cannot be determined with spirography.
Spirometry
Spirometry is a diagnostic method that examines the function of external respiration. The study is carried out using a spirometer. During the examination, the nose is pinched with fingers or with a clamp. To avoid undesirable phenomena ( dizziness, fainting) it is necessary to strictly follow the rules and constantly monitor the patient.
Spirometry can be performed with calm and forced ( enhanced) breathing.
With calm breathing, VC is determined(vital capacity of the lungs)and its components:
- expiratory reserve volume ( after the deepest inhalation, the deepest exhalation is made);
- inspiratory volume ( after the deepest exhalation, a deep breath is taken).
With forced breathing, FVC is determined ( forced vital capacity). For this, a calm exhalation is done, the deepest possible inhalation and then, without a pause, the deepest exhalation is immediately performed. FVC decreases with pathology of the pleura and pleural cavity, obstructive pulmonary diseases, disorders of the respiratory muscles.
Sputum analysis
Sputum is a pathological discharge secreted by the glands of the bronchi and trachea. Normally, these glands produce a normal secretion, which has a bactericidal effect, helps in the release of foreign particles. With various pathologies of the respiratory system, sputum is formed ( bronchitis, tuberculosis, lung abscess).
Before collecting material for research, it is recommended to consume a large volume of water for 8 - 10 hours.
Sputum analysis includes the following items:
- Initially, the characteristics of sputum are analyzed ( content of mucus, pus, blood, color, smell, consistency).
- Then microscopy is performed, which informs about the presence of various shaped elements in the sputum. Detection of microorganisms is possible.
- Bacteriological analysis is carried out to detect microorganisms, possible infectious agents.
- Determination of antibiotic susceptibility ( antibioticogram) allows you to find out whether the detected microorganisms are sensitive or resistant to antibacterial drugs, which is very important for adequate treatment.
Bronchoscopy is an endoscopic examination of the trachea and bronchi. For the procedure, a broncho-fibroscope is used, which is equipped with a light source, a camera, and special parts for manipulation, if necessary and possible.
With the help of bronchoscopy, the mucous membrane of the trachea and bronchi is examined ( even the smallest ramifications). This is the most suitable method for visualizing the inner surface of the bronchi. Bronchoscopy allows you to assess the condition of the mucous membrane of the respiratory tract, identify the presence of inflammatory changes and the source of bleeding, take material for biopsy, and remove foreign bodies.
Preparation for bronchoscopy is as follows:
- the last meal should be 8 hours before the procedure to prevent aspiration of gastric contents in case of possible vomiting;
- premedication is recommended before the procedure ( pre-administration of drugs);
- conducting a detailed blood test and coagulogram before the procedure;
- it is recommended not to take fluids on the day of the study.
- local anesthesia of the nasopharynx is performed;
- a bronchoscope is inserted through the nose or through the mouth;
- the doctor gradually examines the condition of the mucous membrane as the device is inserted;
- if necessary, material is taken for a biopsy, a foreign body is removed or other necessary medical procedure;
- at the end of the procedure, the bronchoscope is removed.
Laryngoscopy
Laryngoscopy is a research method in which the larynx is examined using a special apparatus called a laryngoscope.
There are two methods for performing this manipulation:
- Indirect laryngoscopy... This method is currently considered out of date and is rarely used. The bottom line is the introduction of a special small mirror into the oropharynx and visualization of the mucous membrane using a reflector that illuminates it. To avoid gagging, local spraying with an anesthetic solution ( anesthetic).
- Direct laryngoscopy... This is a more modern and informative research method. There are two options for it - flexible and rigid. In flexible laryngoscopy, the laryngoscope is inserted through the nose, the larynx is examined, and then the device is removed. Rigid laryngoscopy is a more complex technique. During its implementation, it is possible to remove foreign bodies, take material for a biopsy.
Thoracoscopy is an endoscopic research method that allows you to examine the pleural cavity using a special instrument - a thoracoscope. The thoracoscope is inserted into the pleural cavity through a puncture of the chest wall.
Thoracoscopy has several advantages:
- low trauma;
- informativeness
- manipulation can be carried out before open operations to argue the need for a particular type of treatment.
This procedure is less informative when examining the lungs due to the fact that the lung tissue is filled with air, as well as due to the presence of ribs. All this interferes with the examination.
However, there are a number of lung conditions that can be diagnosed with ultrasound:
- accumulation of fluid in the pleural cavity;
- lung tumors;
- lung abscess;
- pulmonary tuberculosis.
Pulmonary dyspnea treatment
Doctors approach the treatment of pulmonary dyspnea in a complex manner, using different methods and means. Treatment is aimed at eliminating the cause of shortness of breath, improving the patient's condition and preventing relapse ( repeated exacerbations) and complications.Pulmonary dyspnea is treated with the following methods:
- Therapeutic, which includes medication and non-drug therapy.
- Surgical method.
Non-drug therapy for pulmonary dyspnea includes:
- rejection of bad habits ( primarily from smoking);
- breathing exercises;
- active immunization against pneumococcus, influenza virus;
- remediation of chronic foci of infection.
Drug therapy
| Group of drugs | Group representatives | Mechanism of action |
| Beta2-adrenergic agonists |
| Relaxation and expansion of the muscular wall of the bronchi. |
| M-anticholinergics |
|
|
| Methylxanthines |
|
|
| Antibiotics |
| Death and suppression of pathogenic flora. |
| GKS (glucocorticosteroids) |
| Anti-inflammatory effect, reducing airway edema, reducing the formation of bronchial secretions. |
Oxygen inhalation ( inhalation). The effectiveness of oxygen inhalation has been proven in cases of pneumonia, bronchial asthma, and bronchitis. Usually, the inhalation procedure lasts about 10 minutes, but the duration may be increased if indicated. You should be careful, as too long a procedure can also harm.
In the absence of the effectiveness of other methods of treatment, they resort to surgical methods of treatment. In some cases, the surgical method is the only chance for the patient to recover.
Surgical treatments for pulmonary dyspnea include:
- Pleural puncture (thoracocentesis) Is a puncture of the pleural cavity. The pleural cavity is located between the two layers of the pleura. The puncture is performed in a sitting position. A place for puncture is selected, disinfected, then local anesthesia is done with a solution of novocaine ( if there is no allergic reaction to it). After that, an injection is made in this area; when a feeling of failure is felt, this means that the parietal pleura has been punctured and the manipulation is successful. Further, the syringe plunger is pulled and the liquid is evacuated ( blood, pus, effusion). It is not recommended to draw out a large amount of liquid at a time, as this is fraught with complications. After removing the needle, the puncture site is treated with an antiseptic and a sterile bandage is applied.
- Thoracotomy- This is an operation in which open access to the organs of the chest is performed through the opening of the chest wall.
- Drainage of the pleural cavity (Bulau drainage) is a manipulation to remove fluid and air from the pleural cavity using drainage.
- Surgical lung volume reduction... The part of the lungs damaged by emphysema cannot be treated and restored. In this regard, an operation is performed to surgically reduce the volume of the lungs, that is, the non-functional part of the lung is removed so that the less damaged part can function and provide gas exchange.
- Lung transplant... This is a very serious operation that is performed for progressive, chronic fibrosing lung diseases. Transplantation is a radical surgical method, which consists in the complete or partial replacement of the diseased lungs of a sick person with healthy ones taken from a donor. Transplantation, despite the complexity of its implementation and therapy after surgery, significantly increases the duration and quality of life of the patient.
Anemia as a cause of shortness of breath
 Anemia is a decrease in the level of hemoglobin, hematocrit, or red blood cells. Anemia can be either a separate disease or a symptom of other diseases. Iron deficiency anemias are most common in clinical practice. Shortness of breath with anemia develops as a result of destruction, disruption of the formation or loss of erythrocytes in the body, a violation in the synthesis of hemoglobin. As a result, oxygen transport to organs and tissues is disrupted and hypoxia is established.
Anemia is a decrease in the level of hemoglobin, hematocrit, or red blood cells. Anemia can be either a separate disease or a symptom of other diseases. Iron deficiency anemias are most common in clinical practice. Shortness of breath with anemia develops as a result of destruction, disruption of the formation or loss of erythrocytes in the body, a violation in the synthesis of hemoglobin. As a result, oxygen transport to organs and tissues is disrupted and hypoxia is established. Causes of anemia
Anemia is a disease that can appear as a result of a wide variety of factors. All etiological factors are characterized by different mechanisms of action, but the effect for all remains common - the state of anemia.Lack of nutrients in the diet most often occurs for the following reasons:
- vegetarian diets;
- long-term diets on exclusively dairy products;
- poor quality food among the population with low incomes.
Lack of iron in the body causes disturbances in the formation of hemoglobin, which binds and transports oxygen to the tissues. Thus, tissue hypoxia and the corresponding symptoms develop. Iron deficiency anemia is called iron deficiency and is the most common anemia.
Impaired absorption of nutrients
In some cases, the necessary nutrients are in the right amount in the diet, however, due to certain pathologies, they are not absorbed in the gastrointestinal tract.
Malabsorption of nutrients more often occurs in the following cases:
- malabsorption syndrome ( malabsorption syndrome);
- gastric resection ( removal of part of the stomach);
- resection of the proximal small intestine;
- chronic enteritis ( chronic inflammation of the small intestine).
There are periods of life when the human body is more in need of certain substances. In this case, nutrients enter the body and are absorbed well, but they cannot cover the metabolic needs of the body. During these periods, hormonal changes take place in the body, the processes of cell growth and reproduction are intensified.
These periods include:
- teenage years;
- pregnancy;
With bleeding, there is a large loss of blood, and, accordingly, erythrocytes. In this case, anemia develops as a result of the loss of a large number of red blood cells. The danger lies in the fact that anemia is established acutely, threatening the patient's life.
Anemia as a result of massive blood loss can lead to:
- trauma;
- bleeding in the gastrointestinal tract ( stomach and duodenal ulcers, Crohn's disease, diverticulosis, esophageal varices);
- blood loss during menstruation;
- donation;
- disorders of hemostasis.
In some cases, anemia appears as a side effect of certain medications. This happens when medication is inadequate without taking into account the patient's condition, or medication is prescribed for too long a period. Typically, the drug binds to the erythrocyte membrane and leads to its destruction. Thus, hemolytic drug anemia develops.
Drugs that can lead to anemia include:
- antibiotics;
- antimalarial drugs;
- antiepileptic drugs;
- antipsychotic medications.
Tumors
The mechanism of anemia in malignant tumors is complex. In this case, anemia may appear as a result of massive blood loss ( colorectal cancer), lack of appetite ( which, in turn, leads to insufficient intake of nutrients necessary for hematopoiesis into the body), taking anticancer drugs that can lead to suppression of hematopoiesis.
Intoxication
Poisoning with substances such as benzene, lead can also lead to the development of anemia. The mechanism consists in increased destruction of erythrocytes, impaired synthesis of porphyrins, damage to the bone marrow.
Genetic factor
In some cases, anemia is established as a result of abnormalities at the genetic level.
Anomalies that lead to anemia include:
- a defect in the membrane of erythrocytes;
- violation of the structure of hemoglobin;
- enzymopathy ( disruption of enzyme systems).
Diagnosis of anemia
Diagnosis of anemia is not difficult. It is usually necessary to conduct a detailed general blood test.CBC indicators important for the diagnosis of anemia
| Indicator | Norm | Change with anemia |
| Hemoglobin |
| Decreased hemoglobin levels. |
| Erythrocytes |
| Decrease in the level of red blood cells. |
| Average erythrocyte volume |
| Decrease in iron deficiency anemia, increase in megaloblastic ( B12 deficiency) anemia. |
| Reticulocytes |
| Increase in hemolytic anemia, thalassemia, in the initial stage of anemia cure. |
| Hematocrit |
| Decreased hematocrit. |
| Platelets |
| Decreased platelet count. |
In order to concretize which type of anemia has, a number of additional studies are used. This is a key point in prescribing treatment, because different types of anemia are treated with different therapies.
To effectively treat anemia, you must adhere to several principles:
- Treatment of chronic diseases that cause anemia.
- Compliance with a diet. Rational nutrition with sufficient nutrients required for blood formation.
- Taking iron supplements for iron deficiency anemia. Iron supplements are usually given orally, but in rare cases they can be given intravenously or intramuscularly. However, with such administration of the drug, there is a risk of developing an allergic reaction, and the effectiveness is lower. Iron preparations include sorbifer, ferrum lek, ferroplex.
- Taking cyanocobalamin ( subcutaneous injections) before the normalization of hematopoiesis and after for prophylaxis.
- Stopping bleeding in case of anemia caused by blood loss by various drugs or with the help of surgery.
- Transfusion ( transfusion) blood and its components are prescribed when the patient is in a serious condition that threatens his life. A reasoned appointment of blood transfusions is necessary.
- Glucocorticoids are prescribed for anemia caused by autoimmune mechanisms ( that is, antibodies are produced against their own blood cells).
- Folic acid preparations in tablets.
- an increase in hemoglobin levels in the third week of treatment;
- an increase in the number of red blood cells;
- reticulocytosis on days 7-10;
- disappearance of symptoms of sideropenia ( iron deficiency in the body).

Why does shortness of breath appear during pregnancy?
 Most often, shortness of breath during pregnancy occurs in the second and third trimester. As a rule, this is a physiological state ( which is not a manifestation of the disease).
Most often, shortness of breath during pregnancy occurs in the second and third trimester. As a rule, this is a physiological state ( which is not a manifestation of the disease).The onset of shortness of breath during pregnancy is easy to explain, given the stages of development of the baby in the womb.
During pregnancy, shortness of breath occurs for the following reasons:
- Shortness of breath as a compensatory mechanism... Shortness of breath appears as a mechanism for the body to adapt to increased oxygen demand during pregnancy. In this regard, changes occur in the respiratory system - the frequency and depth of breathing increase, the work of the respiratory muscles increases, the VC increases ( vital capacity of the lungs) and tidal volume.
- Hormonal adjustment in the body also affects the appearance of shortness of breath. For the normal course of pregnancy, changes in the production of hormones occur in the body. So, progesterone ( a hormone that is produced in large quantities by the placenta during pregnancy), stimulating the respiratory center, helps to increase pulmonary ventilation.
- Increased fetal weight... With an increase in fetal weight, the uterus increases. The enlarged uterus gradually begins to press on the organs located nearby. When pressure begins on the diaphragm, breathing problems begin, which are primarily manifested by shortness of breath. Shortness of breath, as a rule, is mixed, that is, it is difficult to inhale and exhale. In about 2 to 4 weeks, changes occur in the body of a pregnant woman, which also affect the breathing process. The uterus descends 5 to 6 centimeters, which makes breathing easier.
The appearance of pathological shortness of breath during pregnancy can lead to:
- Anemia- This is a condition that often appears during pregnancy. Due to disorders associated with hemoglobin ( violation of synthesis, insufficient intake of iron into the body), oxygen transport to tissues and organs is disrupted. As a result, hypoxemia occurs, that is, a low oxygen content in the blood. Therefore, it is especially important to monitor the level of red blood cells and hemoglobin in a pregnant woman in order to avoid complications.
- Smoking... There are many reasons for the appearance of shortness of breath when smoking. First, there is damage to the mucous membrane of the respiratory tract. Also, atherosclerotic plaques accumulate on the walls of blood vessels, which contributes to impaired blood circulation. In turn, impaired blood circulation affects the breathing process.
- Stress is a factor that contributes to an increase in the respiratory rate and heart rate, subjectively felt as a lack of air, a feeling of tightness in the chest.
- Respiratory system diseases (bronchial asthma, bronchitis, pneumonia, COPD).
- Diseases of the cardiovascular system (cardiomyopathy, heart disease, heart failure).
- high temperature;
- dizziness and loss of consciousness;
- cough;
- pallor or cyanosis;
- headache;
- tiredness and malaise.
Why does shortness of breath appear with osteochondrosis?
 Most often, shortness of breath occurs with cervical osteochondrosis and osteochondrosis of the thoracic spine. In connection with osteochondrosis, breathing disorders are established and a feeling of lack of air appears. Shortness of breath with osteochondrosis can have different mechanisms of occurrence.
Most often, shortness of breath occurs with cervical osteochondrosis and osteochondrosis of the thoracic spine. In connection with osteochondrosis, breathing disorders are established and a feeling of lack of air appears. Shortness of breath with osteochondrosis can have different mechanisms of occurrence. Shortness of breath with osteochondrosis develops most often for the following reasons:
- Reduced space between vertebrae... Due to degenerative changes ( structural irregularities) of the vertebrae and the spine as a whole, thinning of the intervertebral discs gradually occurs. Thus, the space between the vertebrae is reduced. This, in turn, contributes to the appearance of pain, feelings of stiffness and shortness of breath.
- Displacement of the vertebrae... With the progressive course of the disease, dystrophic changes ( characterized by cell damage) in the tissues can lead to displacement of the vertebrae. The displacement of different vertebrae can lead to characteristic consequences. Shortness of breath, as a rule, forms when the first thoracic vertebra is displaced.
- Compression of blood vessels... With a decrease in the space between the vertebrae or their displacement, the vessels are compressed. Thus, the blood supply to the diaphragm, which is the main respiratory muscle, becomes problematic. Also, with cervical osteochondrosis, the vessels of the neck are compressed. At the same time, the blood supply to the brain deteriorates, the vital centers in the brain are suppressed, including the respiratory center, which leads to the development of shortness of breath.
- Pinched or damaged nerve roots can lead to severe pain, which is accompanied by difficulty breathing and shortness of breath, especially when inhaling. Pain in osteochondrosis limits breathing.
- Deformation ( structural disturbance) chest... In connection with the deformation of individual vertebrae or parts of the spinal column, deformation of the chest occurs. In such conditions, breathing is difficult. Also, the elasticity of the chest decreases, which also limits the ability to breathe fully.
To prevent the appearance of shortness of breath in osteochondrosis, you must adhere to the following rules:
- timely diagnosis of osteochondrosis;
- adequate drug treatment;
- physiotherapy and massage;
- physiotherapy;
- avoidance of prolonged stay in one position;
- matching bed and pillows for quality rest during sleep;
- breathing exercises;
- avoiding a sedentary lifestyle;
- avoiding excessive physical exertion.
What to do if a child has shortness of breath?
 In general, shortness of breath in children can be caused by the same causes as in adults. However, the child's body is more sensitive to pathological changes in the body and reacts to the slightest changes, since the child's respiratory center is quite easily excitable. One type of reaction of the child's body to various factors ( stress, physical activity, increased body temperature and ambient temperature) is the appearance of shortness of breath.
In general, shortness of breath in children can be caused by the same causes as in adults. However, the child's body is more sensitive to pathological changes in the body and reacts to the slightest changes, since the child's respiratory center is quite easily excitable. One type of reaction of the child's body to various factors ( stress, physical activity, increased body temperature and ambient temperature) is the appearance of shortness of breath. Normally, the child's respiratory rate is higher than that of adults. For every age group there are breathing rates, so don't panic if your baby's breathing seems to be elevated. Perhaps this is just the norm for his age. Respiratory rate is measured at rest, without prior exercise or stress measurement. It is best to measure the respiratory rate while the baby is asleep.
Respiratory rate norms for children of different age groups
| Child's age | Respiratory rate |
| Up to 1 month | 50 - 60 / min |
| 6 months - 1 year | 30 - 40 / min |
| 1 - 3 years | 30 - 35 / min |
| 5 - 10 years old | 20 - 25 / min |
| Over 10 years old | 18 - 20 / min |
If a deviation from the norm in the frequency of respiratory movements is noticed, do not ignore it, as this may be a symptom of the disease. It is worth contacting a doctor for qualified medical help.
If a child develops shortness of breath, you can consult a family doctor, pediatrician, cardiologist, pulmonologist. In order to get rid of shortness of breath in a child, you should find its cause and fight the cause.
Shortness of breath in a child may appear as a result of the following factors:
- rhinitis ( inflammation of the nasal mucosa) can also lead to shortness of breath, making it difficult for air to pass through the airways;
- bronchial asthma, which is manifested by periodic attacks of severe shortness of breath, and the diagnosis of which in childhood is sometimes quite difficult to establish;
- viral diseases ( influenza virus, parainfluenza virus, adenovirus);
- heart disease ( heart defects), which, in addition to shortness of breath, are also manifested by cyanosis, delayed development of the child;
- lung diseases ( pneumonia, emphysema);
- the ingress of a foreign body into the respiratory tract is a condition that requires immediate intervention, since this can very quickly lead to death;
- hyperventilation syndrome, which manifests itself in stress, panic disorder, hysteria; in this case, the level of carbon dioxide in the blood decreases, which, in turn, contributes to hypoxia;
- cystic fibrosis is a genetic disease characterized by serious disorders of breathing and excretory glands;
- physical exercise;
- diseases of the immune system;
- hormonal imbalance.
Can shortness of breath be treated with traditional methods?
 For shortness of breath, traditional medicine can be used. However, you need to be extremely careful. After all, shortness of breath is often a manifestation of serious diseases that can become a threat to human life. Traditional medicine can be used if shortness of breath occurs occasionally and after heavy physical exertion or excitement. If shortness of breath appears when walking or even at rest, you need to sound the alarm. This condition requires immediate medical attention in order to assess the condition of the body, find the cause of shortness of breath and prescribe appropriate treatment. In any case, folk remedies can be used as a separate method of treatment ( if shortness of breath is not a manifestation of a serious illness) and as an addition to the main course of medical treatment.
For shortness of breath, traditional medicine can be used. However, you need to be extremely careful. After all, shortness of breath is often a manifestation of serious diseases that can become a threat to human life. Traditional medicine can be used if shortness of breath occurs occasionally and after heavy physical exertion or excitement. If shortness of breath appears when walking or even at rest, you need to sound the alarm. This condition requires immediate medical attention in order to assess the condition of the body, find the cause of shortness of breath and prescribe appropriate treatment. In any case, folk remedies can be used as a separate method of treatment ( if shortness of breath is not a manifestation of a serious illness) and as an addition to the main course of medical treatment. Traditional medicine has many remedies and methods for the treatment of shortness of breath, which have different mechanisms of action. Such funds can be taken in the form of solutions, tinctures, teas.
The following traditional medicine methods can be used to treat shortness of breath:
- Cranberry infusion. 5 tablespoons of cranberries must be poured with 500 ml of boiling water, let it brew for several hours, then add 1 teaspoon of honey. The prepared infusion should be drunk within 24 hours.
- Wormwood infusion. To prepare the infusion, you need to pour 1 - 2 teaspoons of wormwood with boiling water, let it brew for half an hour. After readiness, the infusion is taken 1 teaspoon half an hour before meals 3 times a day.
- Astragalus root infusion prepared on a water basis. To do this, take 1 tablespoon of dried and chopped Astragalus root and pour boiling water over it. Then you need to let the mixture brew for several hours. Ready tincture is taken 3 times a day, 3 tablespoons.
- A mixture of honey, lemon and garlic. To prepare the mixture, add 10 peeled and chopped heads of garlic to 1 liter of honey, and squeeze the juice from 10 lemons. Then it is necessary to tightly close the container in which the mixture is prepared and put it in a dark place for 1 - 2 weeks. After that, the medicine is ready for use. It is recommended to drink 1 teaspoon of this medication 3-4 times a day.
- Infusion of potato sprouts. First you need to dry well, then grind and crush the raw materials. The dried sprouts are filled with alcohol, infused for 10 days. It is recommended to take the infusion 1 - 3 potassium 3 times a day.
- Motherwort infusion. 1 tablespoon of motherwort should be poured with a glass of boiling water, let it brew for an hour, and then drink half a glass 2 times a day.
- Lemon balm infusion. 2 tablespoons of dried lemon balm leaves are poured with a glass of boiling water and infused for 30 minutes. The remedy is taken 3 - 4 times a day, 3 - 4 tablespoons.
- Infusion of hawthorn flowers. To prepare the infusion, 1 teaspoon of hawthorn flowers is poured with 1 glass of boiling water, infused for 1 - 2 hours. After readiness, the infusion is taken 3 times a day for 1/3 cup.
By the nature of this symptom, a lot can be said: the level at which the difficulty in breathing arose, how great the obstacle is. This information will allow you to quickly make the right decision and save a person's life.
Shortness of breath happens:
- Inspiratory
- Expiratory
- Mixed
It is important to remember that it is almost always necessary to assess the complex of symptoms, as this will allow a more complete assessment of the severity of the condition. Objective signs to consider:
- Skin color: pallor, cyanosis, redness.
- The position of the patient.
- Respiration and heart rate.
- Breathing sound and wheezing.
- Sound of voice and cough.
- The severity of the involvement of the muscles (chest).
Inspiratory dyspnea
Inspiratory dyspnea - difficulty breathing on inspiration with the participation of auxiliary muscles due to an obstruction in the upper respiratory system (pharynx, larynx, trachea).
The main reasons for this problem may be:
- Foreign body of the larynx or trachea.
- Infections that cause swelling, cramping, and profuse mucus or phlegm.
- Diphtheria.
- Allergic reaction (severe cases of Quincke's edema).
In childhood, with inspiratory dyspnea, a foreign body can never be ruled out.
It is extremely important to quickly determine this circumstance, since it is easier to remove the causal object from the upper parts of the respiratory tube.
 Causes of shortness of breath in children
Causes of shortness of breath in children An infectious cause is perhaps the most common. The process can be both in the pharynx and in the larynx:

Diphtheria (in particular of the larynx) is a special case of an infectious process of the upper respiratory tract. This disease is distinguished because it has a number of features: the appearance of fibrin films on the mucous membrane, which subsequently exfoliate and can completely block the access of oxygen to the underlying parts of the respiratory system. This condition is called true croup. As a rule, it is accompanied by a high fever, typical raids are on the pharyngeal mucosa, and may also be accompanied by diffuse swelling of the neck and upper chest.
Allergy is one of the most dangerous causes of shortness of breath and suffocation, as this reaction develops with lightning speed and requires emergency assistance. Most often, involvement of the larynx in the process is a constituent symptom.
Expiratory dyspnea
In this case, an obstacle occurs in the lower parts of the respiratory system - in the bronchi and bronchioles. With expiratory dyspnea, exhalation is difficult, breathing is noisy with wheezing.
- Foreign body.
- Obstructive or bronchiolitis.
- Bronchial asthma.
A foreign body sometimes penetrates low enough and creates a big problem, so it becomes almost impossible to remove it without consequences. This reason cannot be ruled out in young children, adults in a state of alcoholic or other intoxication, as well as in elderly patients.
Obstructive bronchitis is almost always the result of a viral infection.
With this disease, edema and spasm of the walls of the bronchi occurs, as a result of which air enters the lungs, but cannot completely come out back. The situation is aggravated by abundant secretion of viscous mucus. Bronchitis is always accompanied by a cough, expiratory dyspnea may be accompanied by wheezing, in severe cases, wheezing, which can be heard from a distance.
With bronchiolitis, the pathological process develops in the bronchioles. This disease is possible in children under 6 months, less often up to 1 year. Age, prevalence of the process and weak immunity determine the severity of this condition. Expiratory shortness of breath in this case can very quickly become mixed.
Almost everyone knows what bronchial asthma is. One of its manifestations is difficulty in breathing on exhalation during an attack. Also, the characteristics of this condition are cough, forced position of the body, pallor of the skin.

Mixed shortness of breath
Mixed shortness of breath is a general difficulty in breathing on both inhalation and exhalation. The causes can be varied and can be divided into pulmonary and extrapulmonary.
The first group includes all its possible complications. The inflammatory process causes changes in the lung tissue, which leads to the exclusion of whole segments, lobes, and sometimes the entire lung from the act of breathing. A person cannot live without oxygen, so the body tries to compensate for its lack by shortness of breath.
The larger the affected area, the more pronounced respiratory failure.
Mixed dyspnea can occur in extreme cases of stenosing laryngotracheitis, obstructive bronchitis.
There are a lot of extrapulmonary causes, here is a small list of them:
- Lung edema.
- Pneumothorax, hydrothorax.
- Heart failure.
- Intoxication (in particular, infectious toxic shock).
- Metabolic disorders.
- Poisoning with poisons, heavy metals, carbon monoxide.
- Brain trauma with damage to the centers responsible for breathing and heartbeat.
- Vascular pathology,.

In fact, mixed shortness of breath occurs either when a part of the lung (or all) is excluded from the breathing process, or when there is a lack of oxygen for certain needs of our body.
Diagnostics and treatment
If shortness of breath occurs, especially in childhood, it is necessary to urgently seek help from a doctor. Only a hospital or other medical institution will be able to provide qualified assistance aimed at eliminating both the symptom itself and the cause that caused it.
External respiration.
Breathing consists of the phases of inhalation and exhalation, which are carried out in a certain constant rhythm - 16-20 per minute in adults and 40-45 per minute in newborns.
Respiratory rhythm- these are respiratory movements at regular intervals. If these intervals are the same, breathing is rhythmic, if not, arrhythmic. In a number of diseases, breathing can be shallow or, on the contrary, very deep.
There are three types of breathing:
Chest type- Respiratory movements are carried out mainly due to the contraction of the intercostal muscles. In this case, the chest during inhalation expands and rises slightly, and during exhalation it narrows and drops slightly. This type of breathing is typical for women.
Abdominal type- Respiratory movements are carried out mainly due to the contraction of the muscles of the diaphragm and muscles of the abdominal wall. The movement of the muscles of the diaphragm increases the intra-abdominal pressure and during inhalation the abdominal wall is displaced forward. As you exhale, the diaphragm relaxes and rises, which pushes the abdominal wall backward. This type of breathing is also called diaphragmatic breathing. It occurs predominantly in men.
3) Mixed type- Respiratory movements are performed simultaneously by contraction of the intercostal muscles and the diaphragm. This type is most common in athletes.
In case of violation of the satisfaction of the need to Breathe, shortness of breath may appear, that is, a violation of the rhythm, depth or frequency of respiratory movements.
Types of shortness of breath.
Depending on the difficulty of one or another phase of breathing, there are three types of shortness of breath:
1) Inspiratory- Difficulty breathing. This happens, for example, when a foreign body or any mechanical obstacle enters the respiratory tract.
2) Expiratory- Difficulty exhaling. This type of shortness of breath is characteristic of bronchial asthma, when there is a spasm of the bronchi and bronchioles.
3) Mixed - both inhalation and exhalation are difficult. This type of shortness of breath is common in heart disease.
If shortness of breath is severe, it forces the patient to take a forced sitting position - this is called shortness of breath. suffocate. In addition to the types of pathological dyspnea described above, there are physiological shortness of breath that occurs with significant physical exertion.
If the satisfaction of the need to breathe is violated, the frequency of respiratory movements may change. If the frequency of respiratory movements is more than 20, such breathing is called TACHIPNEA, if it is less than 16, it is called BRADIPNEA.
Sometimes shortness of breath is of a certain nature and the corresponding name:
Breath of Kussmaul;
Breath of Biota;
Cheyne-Stokes breath.
|
Types of pathological respiration |
Abnormal breathing changes |
|
Breath of Kussmaul |
Uniform rare breathing cycles with deep noisy inhalation and increased exhalation. |
|
Cheyne Stokes breath |
It is characterized by periodic expiratory delays lasting from several seconds to a minute, shallow breathing in the dyspnoea phase, increasing in depth and reaching a maximum on the fifth or seventh breath, then decreasing in the same sequence and turning into another respiratory pause. Most often it occurs as a result of dysfunction of the nerve centers, increased intracranial pressure, heart failure. |
|
Breath of Biot |
It is characterized by an alternation of uniform rhythmic respiratory movements and long (up to half a minute or more) pauses. It is observed in organic brain lesions, circulatory disorders, intoxication, shock, and other severe conditions accompanied by deep brain hypoxia. |
Thus, the criterion (sign) of external respiration is the frequency and rhythm. Normally, breathing is rhythmic, the frequency of respiratory movements is 16-20 per minute.
Arterial pulse (Ps) is the oscillation of the artery wall caused by the release of blood into the arterial system during one cardiac cycle (systole, diastole).
The main symptom that signals the onset of heart failure, its important and early symptom is cardiac dyspnea. The cause of shortness of breath is often congestive plethora in the lungs, in addition, shortness of breath reflexively occurs with a reduced cardiac output.
Shortness of breath with heart failure, depending on the stage of the disease, can be expressed in three forms:
- Shortness of breath only on exertion.
- Shortness of breath at rest.
- Acute attacks of shortness of breath with or without pulmonary edema.
However, one should not think that any person who has run up to the tenth floor of his house and after that can hardly catch his breath will certainly suffer from heart failure. Of course not. The so-called physiological shortness of breath during physical exertion, especially strong or unusual, is caused by an increased demand for oxygen in the body. And the amount of oxygen entering the body during shortness of breath (in this case - with very deep and rapid breathing) increases 2-3 times.
Only such shortness of breath is considered pathological, which is felt under physical conditions that did not cause it before. In our case: if, having climbed, for example, to the second floor, a person is forced to breathe as often and as hard as if he ran up to the tenth floor. Such a discrepancy between the magnitude of the load and the shortness of breath it causes indicates the need to immediately consult a cardiologist. It should also be borne in mind that shortness of breath is a sign of a congestive phase of heart failure and therefore is one of the first, but not the earliest manifestations of heart failure. Unfortunately, earlier signs are difficult to catch and are not nearly as reliable as pathological shortness of breath.
In addition to the usual shortness of breath, patients with chronic heart failure syndrome often have orthopnea. This is shortness of breath that occurs when a patient with heart failure is lying with a low headboard (the so-called "orthopnea position"). After the patient takes an upright, or at least a half-sitting position, shortness of breath goes away.
An example is the American President Roosevelt, who suffered from heart failure for a long time. It is known that due to breathing problems, Roosevelt even used to sleep in a chair. Orthopnea occurs due to the fact that when the patient is in a horizontal position, the venous blood flow to the heart increases. The appearance of shortness of breath of this type, as a rule, indicates significant disturbances in the circulatory system.
Intense shortness of breath
In especially severe cases, patients with heart failure exhibit a type of dyspnea such as cardiac asthma or paroxysmal nocturnal dyspnea. This is an attack of intense shortness of breath, quickly turning into dyspnea, also most often develops at night, when the patient is in bed. But, unlike orthopnea, shortness of breath does not go away with an upright position. The gradually increasing suffocation is accompanied by a dry cough or cough with discharge of light foamy sputum, excitement, and the patient's fear for his life. With cardiac asthma, severe weakness, anxiety develops, cold clammy sweat appears, the skin acquires an ash-blue color. If signs of cardiac asthma appear, the patient needs immediate medical attention, because this condition is a threat to the life of a patient with heart failure. As a first aid, you can provide an influx of fresh air into the room and comfortably seat the patient with his legs down. With the immediate provision of qualified medical care, an attack of cardiac asthma can usually be relieved.
When there is not enough air - the causes of shortness of breath and how to deal with it
Dyspnea is the medical name for this ailment.
Almost all of us are familiar with the feeling of lack of air when running or climbing stairs to the fifth floor. But there are times when shortness of breath occurs when walking only a few tens of meters or even at rest. If in such situations it became difficult to breathe, then this is a serious matter.
Breathing is a natural process, so we don't even notice it. But we immediately feel if something is wrong with our breathing. Especially when, for no reason at all, we begin to suffocate. The brain receives the appropriate signal - and our breathing quickens, and this process cannot be controlled by consciousness. Its frequency and rhythm, the duration of inhalation or exhalation have changed - in a word, you feel that you are clearly breathing something wrong. This is shortness of breath.
Types of shortness of breath and treatments
In most cases, shortness of breath is associated with hypoxia - low oxygen in the body or hypoxemia - low oxygen in the blood. Which causes irritation of the respiratory center in the brain. The result is a feeling of lack of air, involuntary breathing rate.
There are conventionally distinguished 3 types of shortness of breath: inspiratory shortness of breath (difficult to inhale) - more typical for heart disease; expiratory shortness of breath (difficult to exhale) - most often occurs with bronchial asthma due to spasms; mixed shortness of breath (when both inhalation and exhalation are difficult) - characteristic of a variety of diseases.
The most important method of dealing with dyspnea is the treatment of the disease that caused it. Once the specialist finds out the cause, an effective treatment plan will be determined. For example, for ischemic heart disease and myocardial infarction, treatment with pills is often used. With bronchial asthma - regular treatment with inhalers. Since the main cause of shortness of breath in many cases is low oxygen in the body, oxygen therapy is one way to reduce shortness of breath.
9 reasons - and the same number of treatments
To determine the cause of shortness of breath, it is important to know how quickly it started. It can occur acutely - within minutes, hours, several days, or gradually - over several weeks, months or years. Let's look at the main reasons.
1. Poor physical condition
In principle, in this case, shortness of breath is more normal than a cause for serious concern.
Physiological shortness of breath occurs after you climb stairs or catch up with a bus. The muscles involved in the work remove oxygen from the blood. The brain is trying to cover the resulting oxygen deficiency, that is, it makes us breathe more often. Such shortness of breath is not dangerous in itself, but if you are gasping for breath even after climbing a couple of floors, it's time to think about your physical shape. In physically active and trained people, shortness of breath occurs less often.
What can you do to get rid of this shortness of breath? You need regular aerobic exercise, which leads to an increased respiratory rate and heartbeat. If you don't have time to go to the gym, brisk walks will do. Go down and up the stairs within 3-4 floors.
As you know, intense excitement, anxiety, anger and fear stimulate the production of adrenaline. Once in the bloodstream, adrenaline forces the body to pass a lot of air through the lungs, provoking hyperventilation. Therefore, with serious experiences, the heart rate increases and shortness of breath appears.
What to do? Shortness of breath caused by such strong emotions is, in principle, safe for health. However, for severe panic attacks (and not just in case of shortness of breath from anxiety), it is best to see a doctor. Severe shortness of breath during anxiety may indicate a disease - for example, vascular dystonia.
3. Anemia or anemia
The most common is iron deficiency anemia. Iron ions saturate the blood with oxygen, play an important role in the processes of hematopoiesis. With their lack, hypoxia develops and an emergency protective mechanism is activated - shortness of breath.
This condition is more typical for women, although men often lack iron in the body. The presence of anemia is diagnosed based on the data of a clinical blood test.
What to do to get rid of anemia and shortness of breath at the same time? With a significant decrease in the level of hemoglobin, the doctor prescribes treatment with iron-containing drugs. They must be taken for at least two months and monitored for proper nutrition. Iron is perfectly absorbed from the liver and red meat, but from plant foods, for example, buckwheat or pomegranates, which are considered a panacea for anemia, is rather poor. In order for the iron contained in the preparation or food to be better absorbed, vitamin C is also prescribed.
This is no longer just insufficient training, but a serious disease that requires a lot of effort from a person to improve his health. At the same time, the danger is not the external fat on the thighs or buttocks, but the internal one, since obesity is not just a cosmetic defect.
A layer of fat envelops the lungs and heart, preventing a person from breathing normally. In addition, in obese people, the heart bears increased stress, since it needs to pump blood into a large fat pad. Therefore, less oxygen is supplied to important organs.
The solution to the problem is one - to get rid of fat under the supervision of a doctor. Do not start with vigorous workouts in the gym - chances are high that you will simply pass out.
5. Pulmonary diseases
Shortness of breath, which occurs with diseases of the respiratory organs, is of two types. Inspiratory - when there is difficulty in inhaling as a result of clogging of the bronchi with mucus or with lung tumors, and expiratory - there is difficulty in exhaling as a result of spasms that occur with bronchial asthma.
To determine the causes of pulmonary dyspnea, it will be necessary to conduct an examination and treatment under the supervision of a specialist pulmonologist. The minimum of studies is a chest x-ray, a clinical blood test, spirography (a study of lung function by graphically recording changes in their volume over time during respiration). In especially severe cases, for example, for the diagnosis of tumors or tuberculosis, other methods are also used. You will probably need bronchoscopy and computed x-ray tomography. Well, as already mentioned, you will need to be treated by a pulmonologist.
6. Ischemic heart disease
In this case, shortness of breath is manifested by a feeling of lack of air. In general, shortness of breath is as common a symptom of coronary heart disease as constricting pain in the left side of the chest.
What to do? If you have shortness of breath and severe chest pains for the first time, call an ambulance right away. In men, especially young men, coronary heart disease sometimes manifests itself for the first time with myocardial infarction. When providing first aid, the scope of research is usually limited to a cardiogram, and after that, a cardiologist decides on the examination and treatment.
7. Congestive heart failure
The early signs of this ailment are quite difficult to catch - usually this is done with the help of special examinations.
With congestive heart failure, shortness of breath is always accompanied by a forced position of the patient. It occurs in a person lying on a low pillow, and disappears when the patient assumes a seated position - orthopnea. For example, US President Roosevelt slept in a sitting position in a chair for this very reason. This shortness of breath occurs due to increased blood flow to the heart in the supine position and overflow of the heart chambers.
Treating shortness of breath in heart failure is not an easy task, but experienced cardiologists and modern medications can sometimes work wonders.
8. Cardiac asthma or paroxysmal dyspnea
Such a sudden shortness of breath, developing into choking, often appears at night. Unlike the previous cause - orthopnea (forced position) - in this case, shortness of breath does not go away either in a sitting or standing position. The person becomes pale, moist rales appear in the chest, and the lungs begin to swell. Such a condition threatens the patient's life, so an ambulance should be called immediately.
Usually, promptly performed treatment is effective and eliminates an attack of cardiac asthma. In this case, the patient will need to regularly visit a cardiologist, since only competent treatment of cardiovascular diseases will maintain health in a normal state.
9. Pulmonary embolism
Almost the most common cause of shortness of breath is deep vein thrombophlebitis. At the same time, a person does not always have varicose veins on the surface of the skin, which would give a bell to consult a doctor. The insidiousness of deep vein thrombophlebitis is that the first episode proceeds quite easily - the leg swells slightly, pains and cramps appear in the calf muscle - the sensations are just like stretching, and they are not prompted to be examined by a doctor. The problem is that after that, blood clots appear in the veins of the problem limb, which can move into the pulmonary artery and block the lumen in it. And this, in turn, leads to the death of a portion of the lung - infarction pneumonia.
Signs of pulmonary embolism are severe shortness of breath, stabbing pains in the chest, and a painful cough that appears sharply against the background of normal health. In especially severe cases, a person's face turns blue.
Modern methods of medicine effectively treat this serious disease, however, it is better not to bring thromboembolism to the stage, but to seek medical help in time for any suspicion of a pathology of the veins of the lower extremities. Signs can include swelling, heaviness in the legs, and cramps in the calf muscles.
As you can see, shortness of breath appears for many reasons, from those requiring only some lifestyle changes and ending with those that require serious treatment. Fortunately, many conditions can be prevented or significantly alleviated by timely treatment for pulmonary and cardiovascular disease.
Shortness of breath as an important symptom in diseases of the cardiovascular system
# image.jpg Shortness of breath is an important and early sign of heart failure (HF). According to the recommendations of the European Society of Cardiology, HF should be considered as a pathophysiological syndrome, in which, due to one or another disease of the cardiovascular system, the pumping function of the heart decreases, which leads to an imbalance between the hemodynamic need of the body and the capabilities of the heart. The decrease in the pumping function of the heart is absolute and relative. The relative decrease may be due to a primary increase in the metabolic demands of organs and tissues, for example, in thyrotoxicosis, or a decrease in the oxygen transport function of the blood in anemia. The most common causes of HF are acute and chronic myocardial lesions - ischemic heart disease, non-coronary myocardial diseases (myocarditis, cardiomyopathy), arterial hypertension, acquired and congenital heart defects, congenital pericardial diseases (exudative and adhesive pericarditis), pulmonary-arterial hypertensive hypertension, thromboembolism of the pulmonary artery system).
HF can be caused by a violation of both systolic and diastolic function of the ventricles, and depending on the primary localization of the pathological process, it can be left or right ventricular.
Systolic HF. This is the most common type of HF. In 2/3 of cases, HF is caused by ischemic heart disease (CHD), other causes of it are diffuse myocardial lesions (myocarditis, dilated cardiomyopathy).
Diastolic HF. Diastolic HF accounts for 20-50% of all HF cases. Diastolic dysfunction develops in cases when the wall of the left ventricle (LV) thickens with a decrease in its compliance; rare causes are aortic and mitral stenosis, pericarditis. A more rare cause of diastolic heart failure is diseases due to hypertrophy, widespread fibrosis, or infiltrative changes (arterial hypertension, restrictive cardiomyopathy, amyloidosis, etc.).
According to the European Epidemiological Study (Improvement, 2000), dyspnea of varying severity in HF occurs in 98.4%.
Heart dyspnea can be expressed in three forms:
- shortness of breath only on exertion;
- in the form of acute attacks (attacks of suffocation);
- shortness of breath at rest.
Diagnostically, these three forms do not essentially differ from each other, since they are different stages of the same condition.
94.3% of patients complain of rapid fatigue, palpitations - 80.4%. Cough, orthopnea, peripheral edema are less common. The frequency of these symptoms in patients with chronic heart failure does not exceed 73%. Almost all symptoms of HF are also found in other diseases, which accounts for their low specificity. The diagnostic value of symptoms increases when several symptoms are combined. In each case, the diagnosis of HF must be confirmed by physical examination data and instrumental methods.
Objective signs of HF
Orthopnea is a nonspecific symptom. It is observed in heart failure and diseases of the respiratory system. The specificity of orthopnea varies and depends on the clinical condition of the patient. In severe HF, the specificity is 91%.
Listening to the third tone (protodiastolic gallop rhythm) reflects mainly the failure of the right ventricle, it is observed with congenital heart defects, pulmonary hypertension, chronic pulmonary heart disease (CP). It is often detected in patients with decompensation. The specificity of this symptom is high (95%), the sensitivity is low, and is associated with a high risk of hospitalization and mortality.
Listening to the IV tone (the presystolic gallop rhythm indicates LV failure, increased ventricular pressure and the resulting increase in atrial pressure. This symptom is most often determined in hypertension, myocardial infarction, LV hypertrophy. The specificity of this symptom in the diagnosis of heart failure is low (50%).
Swelling of the jugular veins. Swelling of the jugular veins is spoken of when the border of the visible part of the jugular vein is 3 cm or more above the level of the sternum. The specificity of this trait is high and is 95%. It is observed in both right and left ventricular failure (at stage II B of heart failure according to N.D. Strazhesko and V.Kh. Vasilenko), is associated with a high risk of hospitalization and death.
Crepitation is not a specific symptom of HF. It can be heard with HF, pneumonia, distress syndrome. The sensitivity of crepitus is low and in severe heart failure with a stable course is 16%.
Palpitations are one of the early symptoms of heart failure and are associated with the body's response to normalize minute volume with reduced stroke.
Peripheral edema in patients with heart failure is accompanied by other symptoms of fluid retention (nocturia, oliguria, weight gain). Edematous syndrome can occur with hydrothorax, more often right-sided.
An enlarged liver with right ventricular failure precedes the appearance of edema. Ascites appears due to an increase in pressure in the portal vein system.
The absence of clinical signs of HF (tone III, swelling of the cervical veins) is not enough to exclude it. Severe heart failure is also possible in the absence of crepitus in the lungs, swelling of the neck veins, and edema. Therefore, in each case, the diagnosis of chronic heart failure must be confirmed by the data of instrumental and laboratory research methods.
An ECG study often reveals LV hypertrophy and overload, focal changes after myocardial infarction, arrhythmias, often atrial fibrillation. With the help of an ECG, it is impossible to either confirm HF or exclude it. The absence of changes in the ECG in the presence of shortness of breath excludes heart disease with an accuracy of 90%.
The main radiological sign of HF is an increase in the size of the heart (with the exception of adhesive pericarditis) and venous congestion in left ventricular failure. The sensitivity of the latter trait does not exceed 50%. With moderate heart failure, the sensitivity of cardiomegaly is 53-58%, with severe heart failure - 87%. Specificity is 90%.
2D EchoCG - method of choice in the diagnosis of heart failure: it allows to assess both systolic and diastolic function, and also receives important information about the nature of the disease as the cause of heart failure (heart defects, infective endocarditis, fluid in the pericardium, systolic pressure in the pulmonary artery).
The most important parameter, which is determined by echocardiography, is the LV ejection fraction, which in its systolic dysfunction is less than 45%.
Brain natriuretic peptide (BNP) is secreted by the left and right ventricles in response to an increase in their volume or intraventricular pressure. The BNP level is often elevated in patients with high end-diastolic blood pressure, which is the cause of shortness of breath. The BNP level rises in proportion to the severity of HF. By the level of BNP, it is impossible to differentiate diastolic heart failure from systolic. Its level is increased in patients with right ventricular heart failure (cor pulmonale, idiopathic pulmonary hypertension, chronic pulmonary embolism), which limits the ability to distinguish dyspnea in primary right ventricular failure. A low BNP level makes it possible to exclude HF as a cause of dyspnea (at the BNP level<100 пг/мл СН маловероятна; 100-400 пг/мл интерпретация затруднительна, >400 pg / ml the probability of HF is high).
Features of shortness of breath in patients with primary right ventricular failure
In a number of diseases, primary right ventricular failure occurs. This is the entire group of diseases that today are united by the concept of pulmonary heart disease, as well as some congenital heart defects (atrial septal defect, tetrad of Fallot, Eisenmenger's syndrome, atypical confluence of the pulmonary veins, etc.).
There are three groups of diseases leading to the development of chronic pulmonary disease.
Diseases primarily affecting the bronchi and lung parenchyma (COPD, diffuse lung diseases).
Diseases primarily affecting the locomotor apparatus of the chest with limited mobility.
Diseases primarily affecting the vessels of the lungs (idiopathic pulmonary hypertension, post-thromboembolic pulmonary hypertension, pulmonary vasculitis).
To date, pulmonary heart of bronchopulmonary and vascular genesis is distinguished by pathogenesis and clinical manifestations, including the nature of shortness of breath (Table 1).
The mechanism of dyspnea in CLS of bronchopulmonary genesis is associated with impaired ventilation of the lungs (chronic obstructive pulmonary disease) and diffusion capacity of the lungs (interstitial pneumonia, tuberculosis, widespread pulmonary fibrosis, etc.) In patients with vascular forms of CLS due to high pulmonary vascular resistance the stroke volume of the heart ("fixed") decreases, and therefore tissue hypoxia develops.
Differential diagnosis of pulmonary and cardiac insufficiency
Since symptoms such as shortness of breath, cyanosis, and sometimes edema of the lower extremities occur in both pulmonary insufficiency (FN) and HF, first of all it is necessary to differentiate these conditions (Table 2).
From the anamnesis in patients with heart failure, it is known about the presence of heart diseases - defects, coronary artery disease, arterial hypertension, myocardiopathy. Physical examination confirms heart disease: percussion enlargement of the borders of the heart, murmurs; with FN, long-term complaints of a productive cough, frequent pneumonia, tuberculosis, etc. are found. Dyspnea in FN is often expiratory, in HF it is mixed. HF is characterized by peripheral cyanosis, while FN is characterized by central cyanosis. Tachycardia, atrial fibrillation are inherent in HF. The auscultatory picture in FN is characterized by weakened breathing, dry scattered wheezing rales; with heart failure, congestive moist rales are usually heard in the lower-posterior parts of the lungs. ECG and EchoCG in patients with HF show signs of changes in the left and right heart, in patients with FN, signs of hypertrophy and dilatation of the right parts of the heart may and appear after the development of FN.
In heart disease, HF is, as a rule, biventricular in nature; in FN, it is of the right ventricular type.
Changes in the function of external respiration in HF are poorly expressed and relate to a certain decrease in the vital capacity of the lungs, an increase in the heart rate and minute volume of respiration. LN is characterized by pronounced changes in the parameters of external respiration. The saturation of arterial blood with oxygen practically does not suffer in HF; in FN, hypoxemia develops early.
Shortness of breath with congenital heart defects
With congenital heart defects with the discharge of venous blood into the arterial bed (Eisenmenger syndrome, single ventricle, tetrad and Fallot pentad), shortness of breath occurs due to hypoxemia. In such patients, along with shortness of breath, there are a number of complaints associated with organ hypoxia - dizziness, fainting during exertion, pain in the region of the heart of angina pectoris, weakness. On examination, attention is drawn to diffuse cyanosis, fingers in the form of "drumsticks". During the study, characteristic noises, changes in heart sounds are heard. The diagnosis of heart disease is confirmed by echocardiography.
The list of references is in the editorial office.
Shortness of breath is one of the most common symptoms that occurs with different types of ailments. Sometimes this indicator indicates irrational physical activity, and sometimes serious pathological changes in the body.
Shortness of breath can appear in acute, subacute and chronic types. It is characterized by a feeling of lack of air, difficulty breathing in or out and coughing.
In a healthy person, after physical exertion, after a couple of minutes, the respiratory rate returns to normal, and with pathogenic processes, the feeling of discomfort does not leave for a long time.
Etiology
Shortness of breath has characteristic causes of the appearance:
- cardiac pathology;
- hyperventilation syndrome;
- oncological pathologies;
- shortness of breath with poor metabolism.
Factors that can also provoke the appearance of shortness of breath when walking are such reasons as: poor physical shape, excess weight,.
Classification
If shortness of breath manifests itself during exercise, then this is the norm. However, if a symptom is detected in a calm state, you need to consult a doctor.
To determine the possible etiology of shortness of breath, the doctor must determine its type. Clinicians distinguish three types of dyspnea:
- inspiratory;
- expiratory;
- mixed.

Inspiratory dyspnea manifests itself in difficult breathing and is formed on the basis of a decrease in the opening in the larynx, trachea and bronchi. Typical for acute respiratory infections in children, laryngeal diphtheria, pleural lesions and injuries that cause bronchial compression.
The second type - expiratory dyspnea, is detected in a patient with difficulty exhaling. The provoking factor for the development of this form of the disease is a decrease in the opening in the small bronchi. The symptom manifests itself with and.
Severe dyspnea of mixed type is diagnosed with advanced lung disease and.
Based on the clinical picture and the patient's complaints, the doctor can also establish the degree of the disease, which has 5 stages:
- initial - shortness of breath is formed when walking or exercising;
- light - breathing is disturbed when climbing up or when walking fast;
- medium - formed at the usual pace of walking and a person needs to stop periodically to catch his breath;
- severe - shortness of breath when walking is greatly aggravated so that the patient needs stops every few minutes;
- very severe - difficulty breathing at rest.
Shortness of breath with pathology of the respiratory tract
Dyspnea is diagnosed by doctors very often. The symptom is formed because the opening in the airways of the bronchi and the accumulation of viscous contents in them decreases. In this case, expiratory shortness of breath appears, which, with incorrect therapy, only becomes more intense.
If shortness of breath appears from, then the patient suddenly has attacks of suffocation. After a light short breath, the patient begins a noisy and heavy exhalation. When special agents are inhaled, which lead to the expansion of the bronchi, breathing returns to normal. As a rule, such exacerbations provoke exposure to allergens.
Shortness of breath with bronchitis and may occur along with the following symptoms:
- signs - lethargy, sweating,;
- when coughing.
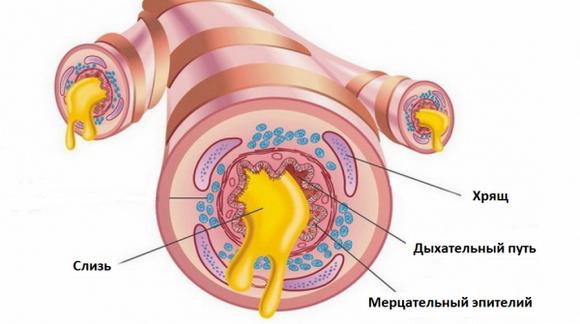
Oncological damage to the respiratory system in the early stages is asymptomatic. As the tumor grows, certain clinical symptoms appear and progress. In addition to shortness of breath, the patient complains of the following symptoms:
- weakness;
- pallor of the skin;
Toxic pulmonary edema is formed on the basis of an infectious lesion, which is accompanied by intoxication or when exposed to the respiratory tract with various toxic substances. At the initial stage of the formation of the disease, shortness of breath in a child and an adult manifests itself rather weakly, breathing quickens a little. After a while, the patient begins to severely suffocate along with gurgling breathing.
Shortness of breath with cardiac pathologies
Cardiac shortness of breath manifests itself from increased pressure in the vessels of the heart. At the initial stages of the formation of the disease, the patient is diagnosed with a slight lack of air during exercise, and with the progression of heart failure, shortness of breath begins to intensify and disturb for a long period of time.
Treatment of shortness of breath in heart failure is prescribed exclusively by a doctor after a diagnosis.
Shortness of breath with poor metabolism
If a patient is diagnosed with a reduced hemoglobin level in the blood, then this may indicate a congenital metabolic disorder, iron deficiency, chronic blood loss, and other serious illnesses that may be accompanied by shortness of breath. In patients with anemia, the following symptoms occur:
- weakness;
- poor memory;
- violation of attention;
- poor appetite;
- disturbed sleep;
- pallor or yellowness of the skin.
Inspiratory dyspnea often occurs with, and overweight. A high content of thyroid hormones leads to an increased contraction of the myocardium, as a result of which the normal pumping of blood through all tissues is impaired. Excess weight is the cause of malfunctioning of many systems of the human body. When it can form, problems with the airway, which will manifest itself as shortness of breath.
Shortness of breath during pregnancy
In the third trimester of pregnancy, the uterus greatly enlarges and begins to put pressure on the diaphragm, as a result of which the respiratory excursion decreases. This process provokes the appearance of shortness of breath.
During pregnancy, anemia is often diagnosed, which also provokes the appearance or worsening of shortness of breath. If a woman has rapid breathing, especially with minor movements, then you need to seek the help of a doctor. It is necessary to treat such an indicator in a very gentle way, so as not to harm the health of the mother and baby.
Shortness of breath in children
Each age category has its own breathing rate norms, by which an unpleasant symptom can be recognized. Such a study should be carried out at a time when the children are sleeping. To measure the number of respiratory movements, you need to put your hand on the chest of the child and count the breaths in and out per minute. It is undesirable to count the respiration rate when feeding and emotionally aroused. At such moments, the child's respiratory rate is much higher and shortness of breath will be physiological.



